
How to reduce autofluorescence
Understand the causes behind autofluorescence and how to deal with this problem.
Immunofluorescence (IF) is a popular antibody-based technique, used to analyse the expression and distribution of proteins in tissues and cells. One of the advantages of using IF over conventional chromogenic stains is the ease of multiplex staining by utilising the distinct emission spectra of separate fluorophores to observe multiple targets on the same slide. IF also has relatively high sensitivity with a wide dynamic range, allowing the observation of low abundance proteins alongside highly expressed proteins, as well as the ability to see protein-protein co-localisations. However, one artifact of IF is the presence of autofluorescence within certain samples, which can often mask the expression of lowly expressed targets or dim dyes. Unfortunately, this makes discerning specific staining from noise in your slide challenging.
What is autofluorescence?
Autofluorescence describes background fluorescence in a tissue that is not attributed to the specific staining of an antigen-antibody-fluorophore interaction. This arises from several causes, and there are steps to minimize its effects in experiments.
Cross-link fixation induced autofluorescence
A common method for tissue fixation is the use of chemical cross-linkers such as formalin. These fixatives work by creating covalent bonds between proteins that bind them together, forming an insoluble mesh that preserves tissue structure. An unfortunate consequence of aldehyde fixation combines aldehydes with amines to form Schiff bases which results in autofluorescence (glutaraldehyde>paraformaldehyde>formaldehyde, PMID: 6404984).
Autofluorescence from such fixation has a broad emission spectrum, occurring across the blue, green and red spectral range (PMID: 24722432). Heat and dehydration of samples can also increase autofluorescence, the effect of which is greater in the red spectrum. The best way to minimize autofluorescence is to fix samples for the least amount of time required. Treatment with sodium borohydride has also been used to minimize this (PMID: 9765122), however it is not well-recommended due to its variable effects. Alternatively, there are other fixatives available, for example using an organic solvent such as chilled (-20 °C) ethanol, which is a good fixative for cells.
 |
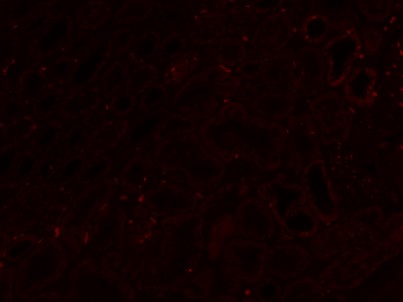 |
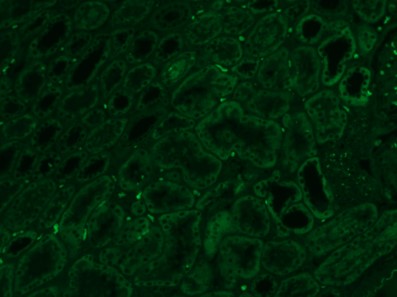
| Figure 1. Endogenous autofluorescence of unstained formalin-fixed paraffin embedded (FFPE) kidney tissue taken using the green (left) and far-red (right) filters. Note how under the far-red filter the background autofluorescence is much less pronounced. | |
Endogenous pigments autofluorescence
Autofluorescence can also occur due to native compounds in tissues. The heme group in red blood cells exhibits broad autofluorescence due to its polyphyrin ring structure which can complicate analysis (PMID: 29058770). The best way to minimize this is to perfuse with PBS prior to fixation. However, PBS perfusion is not always possible for some tissue samples such as post-mortem or embryonic tissue. In some cases, success in reducing autofluorescence has been observed by treating with CuSO4 and NH4CL at a low pH, or bleaching tissues with H2O2.
Other problematic endogenous pigments include collagen, NADH and lipofuscin. Collagen is a highly expressed, ubiquitous structural protein and has an emission spectrum in the blue region around 300-450 nm (PMID: 11830520). NADH is an enzyme essential to many roles in metabolism and its amount increases in metabolically active cells and tissues such as the liver. NADH has an emission spectrum around 450 nm (PMID: 11830520). Therefore, when staining tissue with high levels of compounds such as collagen and NADH (which emit in the blue/green spectrum) choosing a fluorophore with emission spectra in the red and far red regions, such as CoraLite594 and CoraLite 647, will help distinguish specific staining from autofluorescence. Lipofuscin is a granular, lipophilic pigment that accumulates in lysosomes with age in many tissues including skeletal muscles, neurons and the heart. Lipofuscin fluoresces across the spectra, occurring most strongly at 500-695 nm, and thus can be another problematic compound as its granular appearance can be mistaken for specific staining. To negate these effects, Sudan black B, a lipophilic dye, can effectively eliminate this autofluorescence (PMID: 10330448). However, Sudan black B does fluoresce in the far-red channel which must be considered when planning multiplex staining panels.
Summary of autofluorescence troubleshooting
If autofluorescence is a problem in your experiments, these general take-home points may hopefully resolve some issues and “un-shed” some light.
-
Where possible, use alternative to cross-link fixatives or try paraformaldehyde over glutaraldehyde, and always fix for the minimum time required.
-
Sodium borohydride can be used (with mixed results) to decrease formalin induced autofluorescence.
-
Perfuse tissues with PBS prior to fixation to remove the presence of red blood cells.
-
Compounds such as Sudan black B and Eriochrome black T reduce lipofuscin and formalin induced autofluorescence.
-
Use fluorophores that emit in a wavelength further from the autofluorescence compounds in your sample. Typically, far-red wavelength fluorophores such as CoralLite 647 are best for this.
-
Commercially available reagents such as TrueVIEW (VectorLabs), have been shown to reduce autofluorescence from multiple causes.
-
Always perform endogenous tissue controls (no primary or secondary antibody) and primary antibody controls (just secondary antibody) to reveal the level of autofluorescence and non-specific binding in your immunofluorescence experiments.






